Abstract and Introduction
Abstract
Jugular vein aneurysm is a rare morphologic entity. This report describes a case of an asymptomatic internal jugular vein aneurysm that presented as an enlarging mass in the neck. Diagnosis was established with duplex ultrasonography and venography. No thrombus was diagnosed in the aneurysm, but since the patient was uncomfortable with having a tumor in his neck, surgery was performed with resection of the aneurysm and lateral venorrhaphy of the jugular vein.
Introduction
Venous aneurysm is a rare morphologic entity,[1] most frequently described in children.[2,3] In adults, it is described after causing pulmonary embolism when located in the lower extremity,[4] particularly the popliteal vein.[5]
In upper extremity and neck veins, aneurysm is seldom reported since it remains asymptomatic and without clinical relevance.[6] Pain and tenderness have been described as symptoms associated with jugular vein aneurysm, but no serious complications have been reported.
Duplex scanning is sufficient for reliable diagnosis, but three-dimensional ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and venography were described as improvement for morphologic evaluation.[7,8]
We present a case of an asymptomatic internal jugular vein aneurysm (IJVA) that was surgically resected after being described as disturbing for the patient. This was the one-and-only case of a venous aneurysm registered in our university high-volume vascular clinic in 14 years.
A 55-year-old man was admitted to the vascular surgery clinic for a painless mass in the base of the left side of the neck. He recognized it a year before since it enlarged gradually with straining and bending forward. Sixteen years before, he had his left thyroid lobe resected for goiter, but the postoperative course was uneventful. He denied trauma of the neck or a family history. He had no symptoms or history of heart disease.
On physical examination, a 4 x 3 cm soft, rounded, fluctuating mass was seen in the left sternoclavicular fold (Figure 1), which promptly disappeared on compression and enlarged considerably on Valsalva maneuver.

Figure 1.
Enlargement of the aneurysm with straining and bending: arrows depict the outer limits.
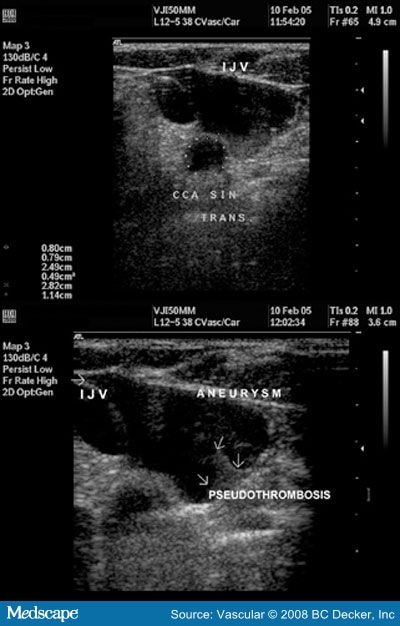
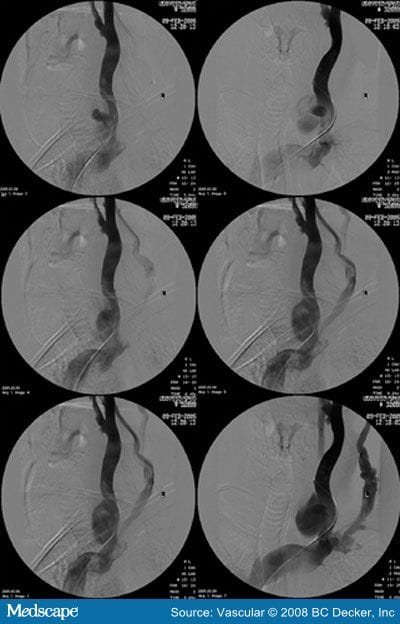
Duplex ultrasonography revealed aneurysmatic formation of the internal jugular vein (Figure 2), measuring 2.82 cm by 1.14 cm in the transverse plane, with high-velocity blood flow within the central part of the aneurysm and much slower near the aneurysmal wall, with the "pseudothrombosis" effect. At venography, 6 to 7 mm communication between the aneurysm and the internal jugular vein was seen (Figure 3).

Figure 2.
Duplex scan: Top: Size of the aneurysm and its relationship to the common carotid artery (CCA) and the internal jugular vein (IJV) in the transverse plane. Bottom: Pseudothrombosis effect (arrows) in the sagittal plane.

Figure 3.
Venography: the aneurysmal neck is seen in the two top images.
Because the patient was very uncomfortable with having a tumor in his neck, surgery was performed through a left supraclavicular approach. After division of the clavicular head of the sternocleidomastoid and omohyoid muscles, the jugular vein and the aneurysm were dissected, and proximal and distal control was obtained (Figure 4). Reconstruction was done with resection of the aneurysm and lateral suture of the jugular vein. No thrombus was found within the aneurysm (Figure 5), and there was no reaction in the surrounding tissue to connect the previous neck surgery with the aneurysm formation. The resected aneurysmal wall was submitted for histologic examination that showed all layers of a normal vein, with fibroblastic proliferation and some mixed muscle layers, with endothelial continuity. No inflammatory infiltrate was seen.

Figure 4.
Dissected aneurysm through the supraclavicular incision with proximal and distal control of the jugular vein.

Figure 5.
Aneurysm opened: an opening of the aneurysmal neck is seen at the bottom of the aneurysm measuring 6 to 7 mm in diameter; no thrombus was found within the aneurysm, and the shiny inner lining of the aneurysmal wall pointed to a true aneurysm.
The operation and the postoperative course were uneventful; and the patient was discharged from the hospital on the third postoperative dayand put on aspirin 100 mg/d. Routine controls were done after 1 month, 6 months, and 1 year. Clinical and duplex scan findings during the 2-year follow-up were satisfactory.
Vascular. 2008;16(5):291-294. © 2008 BC Decker, Inc
Cite this: Jugular Vein Aneurysm - Medscape - Oct 01, 2008.