Objective Pediatric Vision Screening
Objective screening requires less input from children and is faster. With objective screening, the child merely needs to focus on a device long enough to obtain a measurement. One of the most basic forms of objective pediatric vision screening is using the red reflex test to examine young children. The red reflex test looks at the light reflex through an ophthalmoscope. The examiner compares the brightness of the reflexes and determines whether they are normal and equal, otherwise the child is referred to a pediatric ophthalmologist.[10] An abnormal finding could suggest a number of sight-threatening issues including media opacity, strabismus, or significant refractive error.
Another form of objective vision screening is autorefractive screening. There are a number of autorefractors, which can be used to evaluate for amblyopia risk factors. Most of these tests are conducted monocularly and therefore do not screen for strabismus. These devices are used on undilated eyes and will give the user an estimation of the child's refractive error. On the basis of the predetermined referral criteria, the device or examiner can quickly determine whether the child passed the screening or should be referred for further evaluation by a pediatric ophthalmology for a cycloplegic refraction and comprehensive examination. The advantage to autorefractive screening is that it can be carried out not only on verbal children but also on preverbal and nonverbal children as well. It is also much faster than acuity screening.
Currently available autorefractors used for pediatric vision screening include: Grand Seiko binocular autorefractor,[11] Retinomax, and the SureSight. Although the SureSight is specifically marketed as a vision-screening device, both the Retinomax and SureSight autorefractors were validated in the Vision in Preschoolers Study.[12]
Photoscreening is another form of objective vision screening for children. It uses a camera to take binocular images of a child's undilated eyes by looking at the configuration of the crescents of light returning after a flash (red reflex). The devices can estimate refractive error; look for other amblyopia risk factors such as visually significant ptosis, strabismus, and media opacity; and determine which children are at risk for amblyopia. These images can be analyzed by a human interpreter at a reading center, or by software incorporated into the equipment to evaluate the alignment of the eye and estimate refractive error. If significant refractive error or a misalignment seems to be present, it can indicate amblyopia risk factors. If amblyopia risk factors are felt to be present, a referral should be made for the child to be seen by a pediatric ophthalmologist for a cycloplegic examination. Photoscreening has advantages to more traditional eye chart acuity screening, and is particularly useful on younger (age 3 to 5 years), preverbal children (under age 3 years), and nonverbal children.[13] Photoscreening usually takes less than a minute to obtain the necessary images of a child. The only cooperation required is for the child to briefly look at the camera.
Currently available photoscreeners include: iScreen (Fig. 5), MTI (Fig. 6), plusoptiX (Fig. 7), Spot (Fig. 8), and Visiscreen. The MTI photoscreener, iScreen, and Visiscreen use a visible light flash, whereas plusoptiX and Spot utilize infrared light, which is not visible to the child. iScreen, plusoptiX, and Spot have been validated in many recent studies.
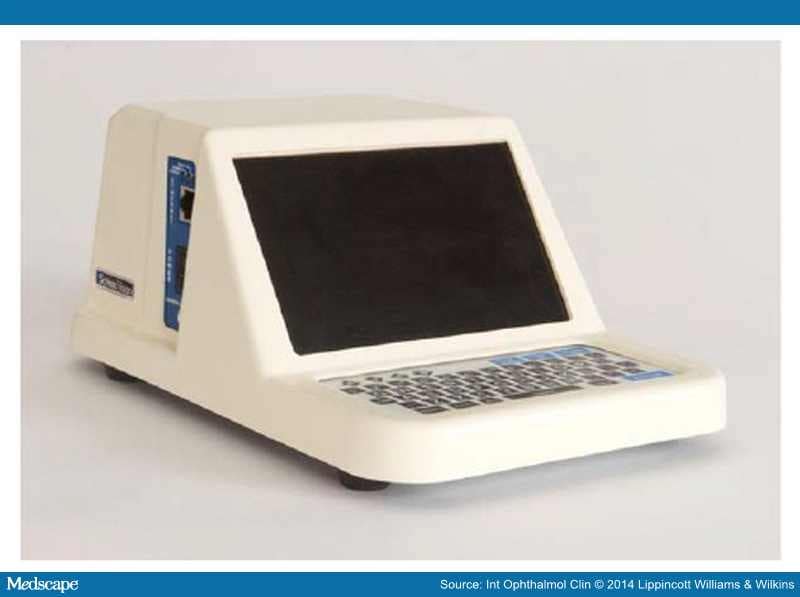
Figure 5.
iScreen photoscreener (photograph courtesy of iScreen Vision). Adaptations are themselves works protected by copyright. So in order to publish this adaptation, authorization must be obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.

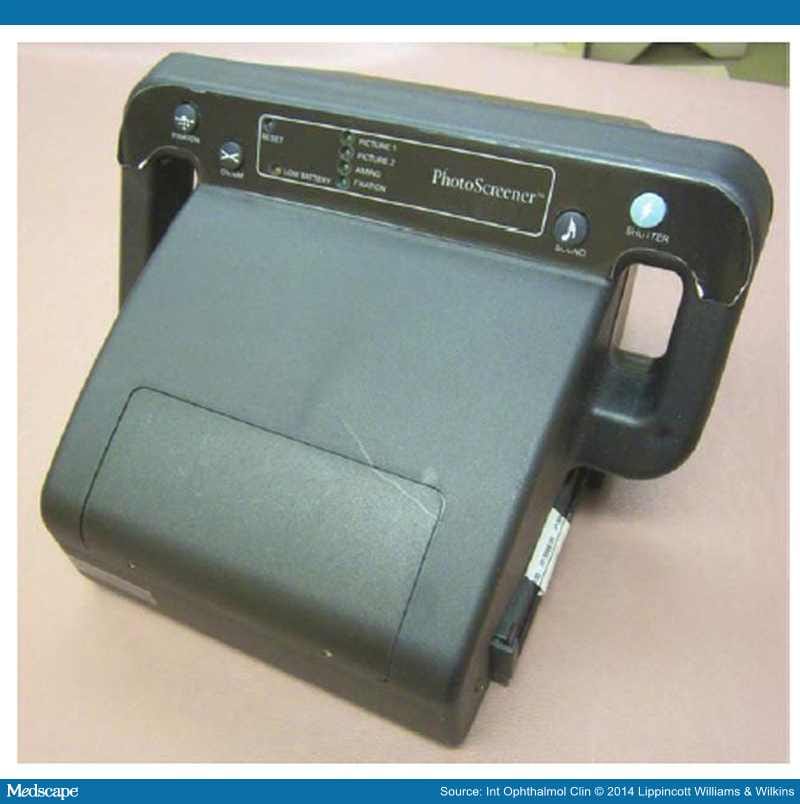
Figure 6.
MTI photoscreener.

Figure 7.
Plusoptix photoscreener (photograph courtesy of plusoptiX Inc., Atlanta, GA). Adaptations are themselves works protected by copyright. So in order to publish this adaptation, authorization must be obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.

Figure 8.
Spot photoscreener (photograph courtesy of PediaVision). Adaptations are themselves works protected by copyright. So in order to publish this adaptation, authorization must be obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.
The iScreen photoscreener was first introduced in 2006. The first generation of the device was an off-axis binocular photoscreener taking 1 image, which is electronically transmitted for remote interpretation. The first generation iScreen was a tabletop device in which the child rests their head against a chin rest. The iScreen 3000, introduced in 2011, has been significantly redesigned and miniaturized.[14] It is now a hand-held device, which takes 2 photographs in rapid succession in 2 axes with a separation of 90 degrees. Aiming beams placed on the child's forehead focus the camera. A blinking fixation light, and sound attract the child's attention. The images are then taken in such rapid succession that the child perceives just 1 flash before a blink. This is an improvement over the analog MTI photoscreener that required lens rotation before taking the second photograph, and prevents differential accommodative effort between photographs. The photograph can be reviewed immediately on the device and if the child is not fixating properly can be retaken. The final image is sent electronically to the company for interpretation, which provides the advantage of a consistent, expert interpretation of the images. A report is e-mailed securely that shows the results of the test and reason for the referral and also includes a picture of the child's eyes.
The MTI photoscreener was first introduced in 1995.[15] The camera uses special high-resolution black and white polaroid style instant film with an off-axis flash that rotates 90 degrees between images. Focus and fixation are similar to the iScreen with aiming beams and a flashing fixation target and noise to attract the child's attention. Two consecutive photographs are taken of each patient resulting in a photograph showing the first image on the top and the second image on the bottom printed on a special high-resolution instant film.[16] On the basis of the shape, size, and location of the crescents, a determination can be made as to whether the child has significant refractive error or strabismus. The MTI is no longer being manufactured but is still in use.
The plusoptiX photoscreener uses an infrared video recorder to obtain images on 3 axes. The device produces a noncycloplegic autorefractive reading, which is then compared with preset referral criteria. If the refractive values exceed the referral criteria, the device will trigger a referral. The referral criteria are user modifiable. The device also creates a scatter plot of the location of the pupillary light reflex and a photographic image of the eyes. A printout is created with the referral advice. The plusoptiX will also trigger a referral if 1 eye deviates by >10 degrees (suggesting strabismus) or if 2 round pupils cannot be seen (such as in a child with an iris coloboma, visually significant ptosis, or if the child will not look at the camera). An advantage to the plusoptiX is the use of infrared light, which is not perceived by the child as a flash. This allows the device to take a number of photographs in multiple axis rather than just 2. It does, however, take longer to acquire the image than the iScreen, which can be an issue with an uncooperative child. The classic plusoptiX is a desktop self-contained Linux-based computer with a hand piece resembling a small radar gun attached. A monitor is provided to view the child during image acquisition. The child fixates on the Smiling "Lucy Face" while noises are playing to attract the child's attention. The spinning infrared beams are also slightly visible that may further attract the child's attention. The device gives audible and visual cues to the tester to focus the device and will not acquire the images until optimal focus is obtained. The device is based originally on the Power Refactor. There have been 4 different variations of the plusoptiX marketed, the S04, S08 (screening models), the S09 and A09 (autorefractor model), and the S12 and A12 handheld model. This newest model has not been as well studied as the desktop units. All desktop models function similarly with similar results.[17] The plusoptiX is marketed by plusoptiX, but was previously comarketed by Pediavision.
The Spot is a new hand-held infrared digital photoscreener developed and marketed by Pediavision.[18] It functions similarly to the plusoptiX but has been significantly miniaturized. Rather than having the infrared elements on the face of the unit flanking the camera aperture, the Spot places the infrared elements below and in front of the camera aperture. The infrared light is then reflected off of a 45% 2-way mirror. The design allows for eye tracking. The device creates a diagram with the location of the eyes, demonstrating any strabismus present and an autorefractive reading. Spot creates a report that can be printed, recommending referral, based on preset criteria.
The Visiscreen is a 35-mm camera with a databack recorder attached to a 500-mm telephoto lens.[19] There is an electronic strobe light located below the lens and a flashing light-emitting diode located above the lens. The camera is mounted on bars ensuring it is exactly 8 feet and 3 inches away from a headrest the patients place their chin on.
Another type of objective vision screening is to utilize visually evoked potential/response. There is currently 1 device available from Diopsys, which estimates visual acuity, or the difference in visual acuity between 2 eyes utilizing a sweep visually evoked potential. The machine analyzes the results and gives the user a pass/refer result. Few validation studies, however, have been conducted.[20]
Int Ophthalmol Clin. 2014;54(3):41-53. © 2014 Lippincott Williams & Wilkins