Timing of Preparation
Reducing the 'runway time' between the last ingestion of bowel preparation agent and colonoscopy improves visualization of the bowel, especially the proximal colon, and enhances the detection of polyps.[10,11] A meta-analysis of five randomized controlled trials performed between 2005 and 2010 involving PEG-based preparations found that split dosing resulted in improved colon cleansing and patient satisfaction when compared with a preparation taken the day prior to examination.[12] Several studies published during the past year further support this view and have even examined same-day preparation.
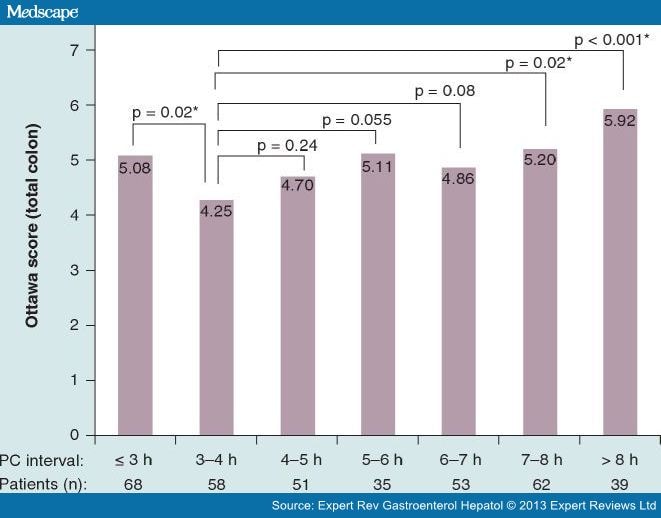
A study by Seo et al. examined the influence of time between last dose of PEG ingestion and start of colonoscopy on bowel preparation quality in 366 subjects.[13] Subjects consumed a low-residue diet for 3 days; 2-l doses of PEG were administered the evening prior to the colonoscopy and another 2-l PEG 2–8 h prior to colonoscopy. The primary outcome was bowel cleanliness using the Ottawa Scale. The best preparation scores, both overall and within each segment, were observed in subjects who consumed their second dose of preparation 3–5 h prior to colonoscopy (Figure 1). Additionally, the study found that the volume of PEG ingested and patient compliance with instructions also correlated with the preparation outcome. While the limitations of this observational single-center study are evident, it serves to reinforce the concepts that split dosing and patient education play important roles in maximizing the quality of bowel cleansing and consequently the quality of colonoscopy.

Figure 1.
The relationship between preparation-to-colonoscopy interval and mean total Ottawa score.
*p < 0.05.
Ottawa: Ottawa Bowel Preparation Scale; PC: Preparation-to-colonoscopy.Reprinted with permission from [13].
Similar findings were reported by another group of Korean investigators who prospectively studied the quality of bowel preparation in 300 subjects undergoing colonoscopy.[14] All subjects were prepared using a 4-l PEG solution. Subjects were requested to record when they began and completed the preparation as well as the procedure start time. They found that a better quality bowel preparation was present in subjects who began their preparation less than 7 h, and completed their preparation less than 4 h, prior to colonoscopy. The authors conclude that the timing of the bowel preparation relative to the time of examination is more important in determining the quality of bowel preparation than the time of examination. The authors conclude that the ideal 'window of opportunity' for achieving the optimal bowel preparation was 4–7 h prior to start of the examination. Comparable studies in western patients are eagerly awaited.
Same-day bowel cleansing for colonoscopy has been practiced in parts of Asia, particularly Japan, for many years. Until recently, this practice was inconceivable to endoscopists in the western world. The trend toward split-dosing has changed this attitude, however, and we are now seeing an increased number of reports describing same-day preparation. Researchers from Mayo Clinic Scottsdale (AZ, USA) retrospectively reviewed the colonoscopy records of 1345 subjects who underwent afternoon colonoscopy.[15] All subjects were instructed to consume a low-fiber diet for 2 days prior to colonoscopy and were given the option of consuming a PEG-based preparation using one of the following dosing schemas: 4 l PEG the evening before, 4 l PEG the morning of, 2 l PEG plus bisacodyl (20 mg) the morning of or 2 l PEG taken the evening before and repeated the morning of colonoscopy. The primary outcome was bowel preparation quality according to the Aronchick score. Multivariate analysis indicated that preparations completed on the same day were more likely to result in a good or excellent preparation compared with the 4 l evening regimen (odds ratio: 7.03; 95% CI: 2.57–19.22; p < 0.001). The secondary outcomes of colonoscopy completion rates and ADR were similar for these three preparations. They concluded that a same-day PEG bowel preparation yields significantly improved colonic preparation for afternoon colonoscopy compared with preparations completed the evening prior to examination.
A study by Longcroft-Wheaten and Bhandari in the UK aimed to compare the efficacy and tolerability of sodium picosulfate in 227 subjects undergoing afternoon colonoscopy who received either two doses the day before and one dose at 8 AM the morning of colonoscopy or two doses on the day of examination (at 7 and 10 AM).[16] The group that received the same-day preparation had better bowel cleansing than the split-dose group with average and excellent preparations observed in 98.4 and 89.5%, respectively (p = 0.0046). Furthermore, patient tolerance was superior with same-day preparation compared with the split-dose regimen. ADRs were similar in both groups.
The optimal regimen for optimizing bowel cleansing, regardless of the purgative agent selected, requires that at least part of the dose be administered within 4–7 h of the examination. This method of split-dosing preparation maximizes bowel cleansing, especially within the proximal colon where flat adenomas and subtle serrated lesions are easily missed if the bowel wall is not well cleansed. It is time for all endoscopists, regardless of what agent(s) they prefer for purgation, to adopt a split-dose regimen for colonoscopy preparation.
Expert Rev Gastroenterol Hepatol. 2013;7(1):77-87. © 2013 Expert Reviews Ltd.