Reconstruction of the Digital Annular Pulleys
General Principles
Often, reconstruction of the annular pulley(s) is necessary after an associated flexor tendon injury and, less commonly, after a closed rupture of the digital pulley. Symptomatic bowstringing of the flexor tendon may require surgical intervention to restore the efficient biomechanical characteristics of the flexor apparatus. Biomechanical studies have suggested that the A2 and A4 pulleys are most crucial to the prevention of tendon bowstringing in the finger.[7,8,9]
Biomechanical studies assessing the outcomes of digital pulley reconstruction have concluded that both the A2 and A4 pulleys should be reconstructed.[7,12,34,35] Reconstruction of the A2 and A4 pulleys was found to restore a more normal combination of angular joint rotation and tendon excursion than other methods of pulley reconstruction.[7] At least 5 mm of each pulley should be reconstructed to help maintain the flexor tendon near the joint center of rotation. Biomechanical studies of the thumb flexor pulley apparatus have concluded that significant tendon bowstringing and altered thumb joint kinematics occur when both the A1 and oblique pulleys are disrupted.[36,37] Normal thumb kinematics were restored when the A1 and/or the oblique pulleys were reconstructed.[37] An intact A2 pulley did not afford an improved biomechanical advantage over a thumb with all pulleys cut.[37] Significantly, the authors concluded that the repair of either the A1 or the oblique pulley was adequate for restoring normal thumb kinematics and that if only one of these two proximal pulleys were injured, reconstruction would be unnecessary.[37]
Tensioning of the graft has been evaluated in conjunction with the effect of the graft source for pulley reconstruction.[24] It was determined that in the range of 0.49 to 1.96 Newtons, the tension of the graft has less effect on the frictional force than does the source of the graft. On the basis of these findings, we recommend that the reconstructed pulley be tensioned to approximately 1 Newton. Since no practical intra-operative tensiometer is routinely available, adequate tensioning of the graft is best approximated in the clinical setting by elimination of tendon bowstringing without restricting tendon excursion through excessive friction.
Tissue Selection
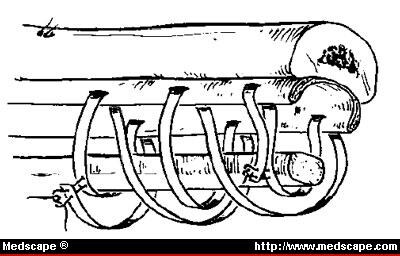
Free tendon grafts are the most common method currently in use for the purpose of digital pulley reconstruction. Bunnell[38] recommended that the A2 and A4 pulley be reconstructed using multiple loops of free tendon grafts placed in the same location as the native pulley. He recommended that the A2 pulley be reconstructed by passing the tendon graft around the proximal phalanx remaining volar to the extensor apparatus. The A4 pulley is reconstructed in similar fashion except that the tendon graft is placed dorsal to the extensor apparatus (Fig 3). The strength of these pulley reconstructions has been shown to be correlated with the number of loops in the tendon.[39,40] Often a right-angled hemostat is useful to pass the tendon graft around the phalanx. The graft is secured in position on the phalanx and to the secondary loops with 4-0 braided Dacron suture using a "belt loop" technique as described by Karev.[41]

Figure 3.
Single loop method of Brunnell[38] as modified by Strickland.
Although extrasynovial tendon grafts, such as palmaris longus, have been used most commonly for pulley reconstruction, recent studies have suggested that intrasynovial donor tendons may be more efficient as a biologic replacement for the absent or incompetent pulley.[23,24,25,42] Basic science investigators have shown that intrasynovial tendon grafts had significantly less frictional resistance to gliding of the tendon than did extrasynvial tendon grafts.[23,24,25,42] Furthermore, the biologic ultrastructure of the intrasynovial tendon grafts promote their survival in the synovial space. Histologic study of these tendons has shown intratendinous canaliculae, which allow intratendinous convection of synovial fluid for nutrition.[43,44] The surface of these tendons is also characterized by a single layer of flattened fibroblasts and hyaluronic acid, both of which may facilitate flexor tendon gliding.[45,46] An animal survival study that evaluated intrasynovial and extrasynovial donor tendons for the purpose of pulley reconstruction showed that intrasynovial donor tendons were associated with less excursion resistance than extrasynovial tendons.[23] More recent clinical studies have concluded that the flexor digitorum longus to the second toe may be safely harvested without significant morbidity.[47,48] This toe flexor or the resected portion of an injured FDS tendon may serve as an intrasynovial donor tendon for flexor pulley reconstruction.
Lister[49] reported on the use of the dorsal wrist retinaculum for the purpose of reconstruction of the annular digital pulleys. Approximately 8 cm of extensor retinaculum is necessary for reconstruction of each digital pulley. He recommended that the under-surface of the extensor retinaculum be oriented toward the tendon to facilitate tendon gliding. Independent biomechanical assessment of this pulley reconstruction concluded that this method is of limited mechanical effectiveness.[39,40] Lister's clinical report concluded that this method of pulley reconstruction was satisfactory for limiting postoperative flexor tendon bowstringing.[49]
The Ever Present Rim. Kleinert and Bennett[50] described a tendon weave technique that uses the rim of the previous pulley to anchor a graft (usually autogenous tendon) (Fig 4). This method of reconstruction has the advantage of creating a long pulley structure that effectively retains the flexor apparatus in close proximity to the bone. Unfortunately, it has also been shown to be one of the weakest of the pulley reconstruction methods.[40]

Figure 4.
"Ever-present" rim technique of Kleinert and Bennett,[50] which uses injured pulley remnant as foundation for graft reconstruction.
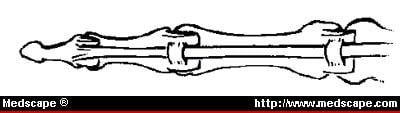
Palmar Plate. Karev[41] recommended the use of the palmar plates for pulley reconstruction. Karev's method (also called the belt loop method) calls for two parallel cuts in the palmar plate of the MP or PI joint. A segment of the plate is raised as a tunnel roof for the passage of a hunter rod or free tendon graft (Fig 5). This method has the advantage of securing the graft near the joint center of rotation. Biomechanical assessment of this method showed that it was less strong and less efficient than the triple loop tendon graft method.[9,51]

Figure 5.
Palmar plate or "belt loop" reconstruction method of Karev.[41]
Flexor Digitorum Superficialis Tenodesis. Strickland[52] has recommended the use of the FDS for the purpose of annular pulley reconstruction. The FDS is harvested leaving the distal insertion intact. A single slip of the tendon is rerouted over the palmar surface of the FDP. The distally based slip of the FDS is secured into the proximal or middle phalanx (depending on which pulley is being reconstructed).
Biomaterials
Hanff and colleagues[29,31,32] have reported on the use of e-PTFE for annular pulley reconstruction in rabbits. Morphologic and biomechanical studies were done 12 and 20 weeks after reconstruction. Pulley reconstructions with e-PTFE were observed to be associated with fibroblast ingrowth into the membrane. Significant flexor tendon adhesions were not reported. The morphologic characteristics of e-PTFE incorporation have been similarly described in an animal survival study.[53] Biomechanical testing showed that the ultimate strength of the e-PTFE pulley reconstructions was similar to that of normal pulleys. Semer et al[54] also reported on the use of e-PTFE for digital pulley reconstructions. They concluded that e-PTFE effectively resists flexor apparatus bowstringing and is not associated with significant adhesion formation.
Researchers reporting on the strength and effectiveness of various pulley reconstruction methods found that the tendon loop constructs were significantly stronger than methods using the extensor retinaculum or a weave through the always-present rim or pulley remnant. The strength of the pulley construct was enhanced by passing a second loop of tendon around the digit, suggesting that improved overall pulley reconstruction strength could be obtained with additional loops of tendon passed around the digit.[40] Lin et al[9] confirmed that additional tendon passes improved the strength of pulley reconstruction. They concluded that a triple loop reconstruction could withstand as much load to failure as a normal annular pulley.[9]
Because it is strong, safe, and effective, the tendon graft loop has become the pulley reconstruction method of choice. Current investigators recommend reconstruction of the A2 and A4 pulleys.[7,8,9] Recent morphologic and biomechanical studies have concluded that intrasynovial donor tendons may have better gliding characteristics than extrasynovial tendon grafts.[23,24,29,42]
John G. Seiler III, MD, 1938 Peachtree St, Suite 603, Atlanta, GA 30309.
J South Orthop Assoc. 2000;9(2) © 2000 Southern Medical Association
Cite this: Digital Flexor Sheath: Repair and Reconstruction of the Annular Pulleys and Membranous Sheath - Medscape - Jun 01, 2000.