Integrating Phages & Phage Cocktails Into Clinical Medicine
The strengths of phages as therapeutic agents[22,50] include:
Their modes of antibacterial action tend to not be affected by mechanisms of bacterial resistance to antibiotics;
Properly formulated and applied phages have sufficient potential to cure bacterial infections, which supports their use as antibiotic substitutes;[8,9,51]
In many cases, phages are numerous, diverse, easily isolated and readily characterized;
A substantial fraction of phages are not inherently toxic to life forms other than their target bacteria;[20]
Collateral damage to normal microbiota, which can be associated with the use of less-specific chemical antibacterials,[4] is avoided.
Nonetheless, there are several challenges that must be addressed prior to widespread adoption of phage therapy. In this section, the authors consider various strategies of phage formulation, including strategies mixing into cocktails, and do so predominantly from the perspectives of both commercialization and regulatory approval.
Striking a Balance in Terms of Activity Breadth
The potential of bacteriophages to remove unwanted bacteria, while not disrupting native microbiota, is an appealing property for a modern antibacterial agent.[20,24,50,52] However, the benefits of using phages or other narrow-spectrum antibacterials[4] must be weighed against the costs associated with identifying the phage susceptibility of pathogens prior to initiation of treatment. The resulting effort contrasts with the relative ease of presumptive treatment, which can be employed when using broader-spectrum antibacterials. In particular, although many pathogens can be rapidly identified to the species level, bacteriophages are often not effective against all strains, even within a single bacterial species.[5] By contrast, activities spanning multiple genera are typical of antibiotics, including various drugs that have entered the 'pipeline' within the last decade.[53] For these reasons, the typical narrowness of a phage's 'spectrum of activity' can be viewed as a key issue to be considered during both development and subsequent medical application of phage therapeutics.
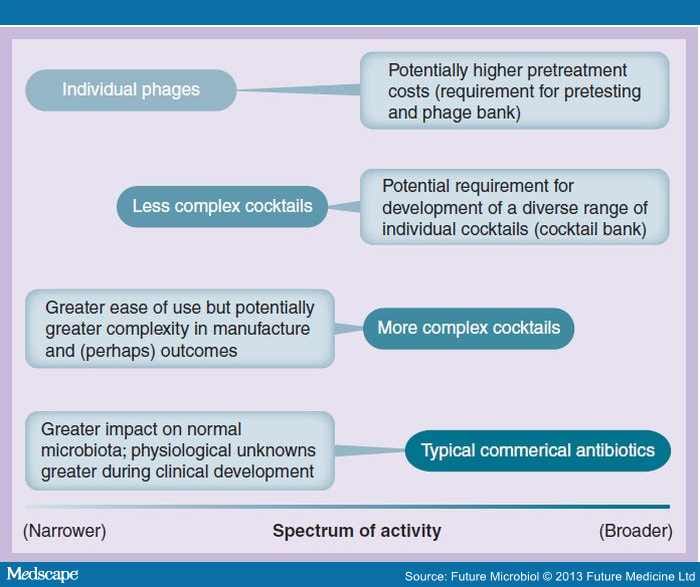
Formulation of phages into cocktails increases their potential to be used presumptively, that is, prior to identification of pathogens (e.g., in terms of phage susceptibility), and the more phages that are included, the greater the potential that there will be sustainable levels of medical as well as commercial demand for a given formulation. However, having too many phages in a cocktail could result in a greater impact on nontarget bacteria, although in most cases this impact is still less than that expected of typical commercial antibiotics. Too many phages per formulation can also result in higher development and manufacturing costs. Figure 1 provides a summary of the burdens associated with overly complex cocktails as a phage therapy strategy (e.g., >50 distinct phages) compared with more personalized monophage therapy. As also indicated in Figure 1, less complex cocktails, for example, two to ten distinct phages, potentially inhabit a middle ground between these two extremes.

Figure 1.
Summary of costs and benefits associated with various phage-based formulations versus typical commercial antibiotics, each as a function of associated spectra of activity.
The suggestion of greater complexities of outcomes refers to the potential for side effects, which, although relatively low on a per-phage-type basis, should be inherently more likely the more phages that are included per formulation. Note that the figure is not intended to imply substantial overlap between the spectrum of activity of more complex cocktails, nor the substantial 'collateral damage' (i.e., bacterial dysbiosis) that can especially result from the use of broader-spectrum chemical antibiotics.
To summarize, while it may be possible to design phage cocktails that are applicable to all possible bacterial targets, including targets that may vary over time, in practice, for a variety of reasons it is usually preferable to generate less complex cocktails. The coverage of less complex cocktails may be incomplete, however, particularly given the limited host range of many phage isolates, as the phage susceptibility of prominent pathogenic strains of bacteria may change over time; for example, as one can observe within the context of phage typing.[54]
Phage Cocktails & Personalized Medicine
The specificity of a therapeutic phage formulation can either be fixed at the point of drug approval or instead can be subject to ongoing development to allow for drug reformulation. More generally, these differences represent distinctions between the 'one-size-fits-all' approach to medical practice versus a more personalized medicine approach.[10,55] In phage therapy terms, this has been described as 'prêt-à-porter' versus 'sur-mesure',[56] which translates to 'ready-to-wear' and, idiomatically, 'custom-made'. Alternatively, a middle ground, which we refer to as 'modifiable', can exist between such 'off-the-shelf' versus 'bespoke'[57] strategies, as we consider in this section (see also the related discussion provided by Verbeken et al.[49]).
The recent push for 'personalized medicine' has resulted in numerous 'omics-based diagnostics that are gradually making their way into clinical practice.[58–61] These technologies can provide a plethora of information with respect to disease predisposition, allowing for the creation of detailed, personalized prevention and treatment plans.[62] In principle, phage therapy could also utilize 'omics technologies, as applied to presumptive bacterial pathogens isolated from patients, to formulate sur-mesure cocktails for those patients. Owing to limitations in our knowledge of phage–bacterial interactions, such an approach could currently only provide a suggestion of which phages may be effective, rather than proof of actual activity. Therefore, in the nearer term, phage-based methods of bacterial identification[54,63] may be used instead.[22] Unless drawn from a well-developed phage bank or otherwise using rapid identification means, such sur-mesure phage therapy can take time to initiate, in the order of days.[56]
Table 2 provides a summary of various general approaches for the treatment of bacterial infections. The phage bank-derived monophage or sur-mesure cocktails are equivalent to personalized phage therapy as mentioned earlier. Preformulated – that is, prêt-à-porter single cocktails – represent the extreme alternative. Here, only a single product is provided for a given infection type. This product would ideally contain a sufficient diversity of phages to have an overall spectrum of activity to include those bacterial pathogens generally known to cause the type(s) of infections being treated. Without personalized sur-mesure approaches, or other alternative phage formulations as back up, however, a lack of target bacteria susceptibility to single cocktails could result in treatment failure without recourse. This prêt-à-porter strategy nonetheless represents what the authors would label as a 'western pharmaceutical model of development' of phage therapy (Figure 2), as it is thought to best fit a combination of constraints imposed by drug regulation and typical medical practice. The prêt-à-porter approach is especially appealing when consistency in drug formulation over time and in different locations is deemed to be particularly desirable.

Figure 2.
Models for implementation of phage therapy.
These consist of either (A) fixed-formulation phage cocktails, (B) cocktail banks or individual phages, or (C) nonfixed formulation cocktails. (A) The fixed-formulation approach ('western pharmaceutical model of development') inherently requires less effort at all stages following formulation regulatory approval as both phage matching and formulation development or modification are avoided. The same approach, however, is also inherently less flexible in terms of responding to bacterial resistance and can be a problematic model towards phage therapy regulatory approval [49]. (B) The phage bank approach is highly flexible but also somewhat labor intensive, especially immediately prior to the commencement of treatment. (C) A single cocktail but modifiable approach represents a middle ground that allows for flexibility in formulation in response to bacterial resistance, but otherwise inherently requires less effort during use. See [56] for additional discussion of many of these concepts.
More than one middle ground exists between these two extremes. The first could involve the preformulation of more than one phage cocktail. Rather than a single cocktail formulated to simultaneously combat multiple species or even genera of possible etiologies of a given infection type, multiple cocktails could be formulated, each with a spectrum of activity that includes, for example, only a single pathogen species. In this case, treatments could be initiated presumptively against the most likely cause(s) of an infection but then could also be followed up with cocktails against different bacterial species if initial treatments were proven to be ineffective. This approach could also be personalized for specific patients; however, rather than individual phages chosen from a phage bank, individual cocktails would be chosen from a 'cocktail bank'. The utility of this cocktail bank approach would ideally be the use of fewer phage types overall in the course of treatment. The costs, however, would be a greater development expense, as well as the production and distribution costs of multiple cocktails.
The second middle ground dispenses with the complexity of multiple cocktails as well as that of strictly personalized medicine, opting instead for a single cocktail, but one that has a formulation that is modifiable over time. This latter approach is exemplified by the experience in the former Soviet Republic of Georgia,[8,57] where prêt-à-porter products are used that are relatively fixed per formulation, but nonetheless are not held completely static over time. These products include 'Pyophage', which contains phages that target E. coli, Proteus, Pseudomonas, Staphylococci and Streptococci and is used to treat infections, such as those from wounds. A different product that is used to treat gastrointestinal infections, 'Intestiphage', instead targets over a dozen gastrointestinal pathogens. These cocktails may be updated twice annually, for instance, by the addition of phages targeting the most prevalent circulating pathogenic strains (in Figure 2C this is what completes the dashed-line loop, thus allowing for ongoing formulation development). In addition to obtaining new phages to include in cocktails, existing phages are also adapted to otherwise phage-resistant strains of target bacteria (see[56] and also above), a process that can be viewed as a means of extending the useful lifespan of otherwise well-characterized and effective phage isolates. To a large extent, these products are also allowed to vary from region to region and producer to producer.
Are 'Modifiable' Antibacterial Strategies Permissible in Western Medicine?
"Ninety years of phage therapy have shown that after a while phage preparations become less effective and need to be updated."
– Pirnay et al. [56]
Is it inherently necessary for steep regulatory costs, as associated with reformulation, to cause phage cocktails to remain static over long time frames? Or, instead, should bacteriophages be treated using a different model from that associated with typical antibacterial drug development? Historically, US FDA regulations have required safety and efficacy testing of each component of drug cocktails.[64] Nonetheless, one alternative model for drug development – which bears similarity to the single cocktail-modifiable approach previously discussed – is employed in the annual reformulation of trivalent influenza vaccines.[56,65] This approach in particular has the utility of not requiring de novo regulatory approval. In this model, individual influenza isolates, at a first approximation, are assumed to behave pharmacologically in a manner that is similar to previously employed influenza vaccines. With phages, this assumption cannot be strictly applied since the genetic variability within phage communities can be vastly greater than that seen even among the rapidly evolving influenza viruses. In addition, while the predominant form of the influenza vaccine is inactivated,[66,67] phages in phage therapy are applied in a live, typically genetically unmodified form. Nevertheless, phages possess two characteristics that might allow for therapeutic development based on an influenza vaccine-like model.
The first of these characteristics is that most phages are not inherently human pathogens and therefore are less in need of either attenuation or inactivation prior to their safe use as drug equivalents. Instead, in many circumstances phages may be viewed as intrinsically nonharmful owing to their long history of replication using hosts that are not humans, mammals, animals or even eukaryotes.[20] The inherently benign behavior of many phages can also be viewed as representing one of the underlying biological reasons that the P100 phage found in the Listex food additive was granted a 'Generally Regarded as Safe' designation by the FDA in 2006[201] as well as for the FDA approval of LMP-102, now known as ListShield™ (Intralytix, MD, USA), also for food treatment.[202]
Not all phage isolates are innocuous.[68,69] Consequently, phages still require substantial characterization prior to their use as therapeutics. The second relevant phage characteristic, therefore, is the potential for bioinformatic methods to rapidly predict phage properties that should be avoided, if possible, in phages used for phage therapy. This approach, following sequencing, in fact provided part of the basis for the P100 Generally Regarded as Safe designation as well as the FDA approval of LMP-102. Ongoing improvements in bioinformatics and other technologies suggest that the day may be approaching where it is phage characterization strategies, such as approaches to genome annotation, that will be subject to basic regulatory approval rather than individual phage isolates themselves. Therefore, we suggest that isolates that meet specific, stringent safety as well as efficacy criteria[13] might be given streamlined regulatory approval based on predefined, highly rigorous procedures rather than de novo, full-blown clinical safety and efficacy trials for all phage isolates proposed to be included in cocktails. We also imagine that the criteria that must be met to gain regulatory approval could differ as a function of proposed use, such as in terms of phage application strategy (per os vs topical vs parenteral) or the bacterium being treated (including being based on severity of infections or effectiveness of alternative available treatments). The chemical as well as physical nature of formulations, such as in terms of buffers, preservatives, osmolarity and pH, by contrast, would probably be required to remain within well-defined ranges, as subject to prior regulatory approval.
It is of interest that a number of these ideas are either in limited use for the influenza vaccine, such as in the case of live attenuation,[66] or instead have been proposed for use. Cold-adapted and therefore nasal-limited and thus attenuated 'master' strains of influenza are literally mated with influenza strains against which a live-attenuated vaccine is sought.[70] Indeed, hybrid strains are also used to produce even inactivated influenza vaccines, as their ability to effectively replicate in embryonated eggs is important to vaccine production. This generation of modified viruses for vaccine production is similar to proposals for creating phage strains that are then modified in terms of which target bacteria they can impact (see [71] and above), though there can be limitations associated with that specific approach for phage cocktail development.[28] Bioinformatics is further suggested as a means of predicting the magnitude of immune responses to different gene variants, and a patient-centered, individual approach is also mentioned in terms of further influenza vaccine development.[72] In other words, improvement of virus-based pharmaceuticals within a streamlined regulatory framework is not without precedent.[73,203]
Licensure of reformulated influenza vaccines in the USA requires a clinical trial to ensure the existence of a potential to generate adequate levels of protective antibody.[74] This requirement is logical as it represents an efficacy check prior to large-scale manufacturing. It can also be viewed as representing close monitoring of the early use of a given vaccine formulation, since individuals given successful vaccination will achieve an outcome (immunity) that is equivalent to subsequently vaccinated individuals. A similar approach undertaken with regard to new phage isolates, however, would have to involve some form of treatment of existing infections. We thus envisage an analogous licensure of reformulated phage products that involves limited testing with close monitoring of outcomes – the latter as an equivalent to Phase IV studies, which involves postmarketing assessment of drug efficacy and safety. While healthy individuals represent the target population for most vaccine testing, it is a comparatively rarer bacterium-infected population that would need to be identified for equivalent phage testing.
Interesting parallels exist between phage therapy and its possible regulation with what are known as 'biopesticides', as well as microorganism-mediated biocontrol agents more generally.[75] As noted by the Environmental Protection Agency (EPA), "Biopesticides are usually inherently less toxic than conventional pesticides … [they] generally affect only the target pest and closely related organisms, in contrast to broad-spectrum, conventional pesticides … [and] often are effective in very small quantities and often decompose quickly".[204] Potentially equivalent to phage therapy, biopesticide use is not necessarily equivalent to that of conventional, chemical pesticides, such that "users need to know a great deal about managing pests." In addition, with regard to biopesticide regulation, it is noted that: "Since biopesticides tend to pose fewer risks than conventional pesticides, EPA generally requires much less data to register a biopesticide than to register a conventional pesticide. In fact, new biopesticides are often registered in less than a year, compared with an average of more than 3 years for conventional pesticides. While biopesticides require less data and are registered in less time than conventional pesticides, EPA always conducts rigorous reviews to ensure that pesticides will not have adverse effects on human health or the environment. For EPA to be sure that a pesticide is safe, the agency requires that registrants submit a variety of data about the composition, toxicity, degradation and other characteristics of the pesticide".[204]
It is notable that phages can be employed within agricultural settings as antibacterial biopesticides.[18] Regulatory standards, however, are not equivalent between the EPA and the FDA, from region to region, nor necessarily between vaccines and antibacterial agents. Nonetheless, these alternative approaches to regulatory approval minimally indicate that frameworks for the regulation of bioactive substances are not monolithic (see [49]).
Strategies for continuous product development within a streamlined regulatory framework could be described as representing a quasipersonalized model of medicine. In this case, 'quasipersonalized' refers to populations or subpopulations of individuals existing at specific points in time or in specific locations, that is, where optimal treatment approaches may vary spatiotemporally. Here, either individual phages or phage cocktails would be 'personalized' to the current and also potentially regional characteristics of the etiology being treated, and this would be rather than strictly to pathogen characteristics as found in individual patients. If successfully developed, we envisage that this modifiable approach could serve as a means by which both the commercial and medical utility of phages may be aligned towards addressing the current need for diverse, safe and abundant antibacterial 'drugs' possessing novel mechanisms of action. Such an approach also basically represents the standard model of phage therapy development employed in the former Soviet Republic of Georgia, where phage therapy has enjoyed both historical and ongoing success in combating bacterial infections.[8,9] Within this framework, further personalization is also possible given a more labor-intensive per-patient matching between etiologies and specific phages or cocktails that also have been subject to the equivalent streamlined approval process – a strategy that is routinely practiced in Poland as well as episodically in Georgia. Alternatively, it has been suggested that "products for bacteriophage therapy deserve their own regulatory framework in Europe".[49] Verbeken et al. also discuss many of the issues considered in this section.[49]
Future Microbiol. 2013;8(6):769-783. © 2013 Future Medicine Ltd.