Article Text

Abstract
Objective Troponin and high signal intensity on T2-weighted (HighT2) cardiovascular magnetic resonance imaging (CMRi) are both markers of myocardial injury in hypertrophic cardiomyopathy (HCM). The interplay between exercise and disease development remains uncertain in HCM. We sought to assess the occurrence of postexercise troponin rises and its determinants.
Methods Multicentre project on patients with HCM and mutation carriers without hypertrophy (controls). Participants performed a symptom limited bicycle test with hs-cTnT assessment pre-exercise and 6 hours postexercise. Pre-exercise CMRi was performed in patients with HCM to assess measures of hypertrophy and myocardial injury. Depending on baseline troponin (< or >13 ng/L), a rise was defined as a >50% or >20% increase, respectively.
Results Troponin rises occurred in 18% (23/127) of patients with HCM and 4% (2/53) in mutation carriers (p=0.01). Comparing patients with HCM with and without a postexercise troponin rise, maximum heart rates (157±19 vs 143±23, p=0.004) and maximal wall thickness (20 mm vs 17 mm, p=0.023) were higher in the former, as was the presence of late gadolinium enhancement (85% vs 57%, p=0.02). HighT2 was seen in 65% (13/20) and 19% (15/79), respectively (p<0.001). HighT2 was the only independent predictor of troponin rise (adjusted odds ratio 7.9; 95% CI 2.7 to 23.3; p<0.001).
Conclusions Postexercise troponin rises were seen in about 20% of patients with HCM, almost five times more frequent than in mutation carriers. HighT2 on CMRi may identify a group of particularly vulnerable patients, supporting the concept that HighT2 reflects an active disease state, prone to additional injury after a short episode of high oxygen demand.
- cardiac troponin
- hypertrophic cardiomyopathy
- exercise, CMR
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In patients with hypertrophic cardiomyopathy (HCM), highly sensitive cardiac troponin (hs-cTn) is elevated in about 25%–50%.1–3 In analogy to other cardiac disorders, the first long-term follow-up data suggest that troponin is associated with adverse outcome in HCM.1
There is limited information about the factors that contribute to troponin release in this particular group of patients. Troponin concentrations have been related to left ventricular (LV) mass and the presence of imaging signs of myocardial injury.2–5 Importantly, it is widely appreciated that the hypertrophic phenotype in HCM is related to pathophysiological abnormalities in vasculature, myocardial structure and function,6 7 which may all contribute to the occurrence of myocardial ischaemia.8 9 Cardiac magnetic resonance imaging (CMRi) studies have correlated areas of ischaemia with segmental late gadolinium enhancement (LGE) and high signal intensity on T2-weighted imaging (HighT2).10–12 HighT2 has been demonstrated to be strongly associated with elevated troponin in HCM and is considered to represent an active state of disease.4 13
In the abovementioned context, episodes of high oxygen demand may pose a challenge and could result in additional myocardial injury. However, whereas studies in ischaemic heart disease and even in healthy individuals have already studied postexercise troponin release and contributing variables,14–16 data in HCM is limited.17 18
With mutation carriers without hypertrophy as a reference group, we aimed to assess and compare the proportions of patients with HCM with a troponin rise after a symptom limited bicycle stress test. In follow-up on studies that addressed troponin concentrations at rest and associated variables, we focused on clinical and CMRi variables that were associated with a postexercise troponin rise.
Materials and methods
Study population
Between 2008 and 2014, subjects were enrolled and participated in a Dutch multicentre study on CMRi and biomarkers in patients with HCM and mutation carriers without hypertrophy. Three specialised HCM outpatient clinics, that is, the Albert Schweitzer Hospital, Dordrecht, the Erasmus Medical Center, Rotterdam, and the Radboud University Medical Center, Nijmegen, the Netherlands, collaborated in this project.4 Two groups were identified: (1) patients with clinical HCM, defined echocardiographically with a maximal wall thickness of ≥15 mm or ≥13 mm in case of a proven sarcomeric gene mutation and (2) carriers of a sarcomeric gene mutation, without echocardiographic evidence of hypertrophy.
Exclusion criteria were cardiac hypertrophy with a known cause other than a sarcomeric gene mutation; a history of coronary artery disease, myocardial infarction or stroke; a history of septal reduction therapy; a contraindication to perform exercise testing. The study complies with the Declaration of Helsinki and the protocol was approved by the local ethics committee, and all participants gave written informed consent. Participants were not involved in the design or conduct or reporting or dissemination of our research.
Study protocol
At the day of the exercise test, New York Heart Association class, medication use, vital parameters, and a resting ECG were recorded and renal function was assessed prior to CMRi. After CMRi, participants performed a bicycle exercise test, with blood samples drawn at baseline and 6 hours after stress testing.
Bicycle exercise test
The exercise protocol prescribed an increase of exercise load of 10 W every minute. During exercise blood pressure, heart rate and ECG were recorded every 2 min. Participants were asked to continue intake of heart rate reducing medication until the day before the test.
The test was symptom limited or terminated in case the participant was no longer able to maintain a cycling frequency above 40 rpm. In all other cases, the test was continued until a workload of 30 W above the expected maximum.
Measurement of serum cardiac troponin T
After processing, serum samples were stored at –80°C until further analysis. For determination of cardiac troponin T the hs-cTnT assay was used (Roche Diagnostics). This test has a limit of blank of 3 ng/L, a limit of detection of 5 ng/L and a 99th percentile upper reference limit of 14 ng/L. The coefficient of variation is reported to be less than 10% at 13 ng/L. A troponin level ≥14 ng/L is called elevated.
A troponin rise was defined according to the level of imprecision. In case of a baseline troponin concentration <13 ng/L, an increase of more than 50% was required to qualify for a rise in troponin; for baseline values ≥13 ng/L, a >20% increase was defined as a rise in troponin.
CMRi
CMRi studies were performed on a 1.5T MR imaging system (Philips Achieva, Philips Healthcare, Best, The Netherlands; or Siemens Avanto, Siemens Health Care, Erlangen, Germany) and analysed according to a previously described protocol.4 In short, breath-hold triple inversion-recovery T2-weighted images with fat suppression were obtained to assess the presence of oedema. Second, steady-state free precession cine imaging was used to quantify LV geometry. Finally, 10 min after administration of 0.2 mmol/kg contrast medium (Dotarem; Guerbet, Gorinchem, The Netherlands), the presence of LGE was assessed with T1-weighted inversion-recovery imaging.
Images were analysed offline with the use of Qmass software (Version 7.5; Medis, Leiden, The Netherlands) by two observers unaware of patient characteristics. LV mass was calculated by subtraction of endocardial from epicardial volume and multiplication by 1.05 g/cm3. LV mass was normalised to body surface area; an increased LV mass was defined as >91 g/m2 for men and >69 g/m2 for women.19 A per segment analysis was performed automatically to assess LV maximal wall thickness (MWT) at end diastole. According to the American Heart Association-model, all 17 LV segments were visually analysed by two observers (JB, FG), who assessed both the presence of HighT2 and LGE, independent of each other, and unaware of troponin results. In case of a discrepancy between observers, a third reader independently re-evaluated all images for final adjudication (HD).
Statistical analysis
Continuous variables were described as means±SDs or medians with IQRs, whenever appropriate. Categorical variables were expressed as frequencies and percentages. To compare two independent groups, the Student’s t or Mann Whitney U test were used for continuous variables, and χ² or Fisher exact test for dichotomous variables, whenever appropriate. The difference between median troponin concentrations pre-exercise and postexercise was tested with the Wilcoxon signed rank test.
Patients with clinical HCM with and without a postexercise troponin rise were compared. Multivariable logistic regression was performed for variables univariably associated with a troponin rise (p<0.10) using stepwise forward logistic regression (p-entry: 0.05 and p-removal: 0.10). First, a model composed of baseline characteristics (clinical and exercise variables) was evaluated. Then, information on the pre-exercise hs-cTnT concentration was added. Finally, CMRi characteristics were included. To assess calibration of the models, we used the Hosmer-Lemeshow test. To assess the performance of each model C-statistics were calculated. P<0.05 indicated statistical significance. All analyses were performed using IBM SPSS22.
Patient and public involvement
Patients were not involved in designing of, recruitment to, or conduct of the study. As our study data are hypothesis generating with potential future clinical consequences regarding exercise in patients with HCM, our results will have impact on future study designs that might include patient-tailored exercise programmes.
Results
Pre-exercise characteristics
The final study population consists of 180 out of a total of 194 participants: in 10, troponin test results were unavailable, in 1 data of the exercise test was incomplete and 3 were unable to perform the exercise test.
In total, there are 127 patients with clinical HCM, with 93% in New York Heart Association class 1–2. The control group consists of 53 mutation carriers without hypertrophy. A mutation was identified in 66% of patients with a clinical HCM. In 81% of cases, the mutation was located in the MYBPC3 gene and for mutation carriers without hypertrophy in 74%.
Table 1 shows baseline characteristics of both groups. Patients with HCM were older and more often male than mutation carriers, and they more often reported symptoms and medication use. In patients with HCM, the interventricular septum (p<0.001) and posterior wall (p<0.001) were thicker, and the median left atrial diameter was larger compared with mutation carriers (p<0.001).
Baseline characteristics of patients with clinical HCM and mutation carriers without left ventricular hypertrophy
Bicycle exercise test
Table 1 shows exercise test parameters of the participants. Patients with HCM achieved lower absolute and relative exercise loads than mutation carriers (p<0.05). Accordingly, in patients with HCM, the duration of exercise was shorter than in mutation carriers and the proportion that did not reach 80% of the expected load was higher (p<0.05). Patients with HCM had lower heart rates at maximum exercise (p<0.001) and lower heart rate pressure products than mutation carriers (p=0.04).
Postexercise troponin rise
The proportion of patients with HCM with a significant troponin rise 6 hours after exercise was 18% (23/127), compared with 4% (2/53) in mutation carriers (p=0.01). In patients with HCM, the pre-exercise median troponin concentration was 8.3 ng/L vs 9.9 ng/L postexercise (p<0.001). Pre-exercise levels ≥14 ng/L were seen in 24%, and postexercise, this was observed in 32% (table 2). Among mutation carriers, there were no individuals with a hs-cTnT ≥14 ng/L, neither before nor after exercise.
Highly sensitive cardiac troponin T results in patients with clinical HCM and mutation carriers without left ventricular hypertrophy
Contributors to postexercise troponin rise in HCM
Table 3 displays clinical, biomarker and imaging characteristics in association with a troponin rise.
Clinical
Patients with clinical HCM with a postexercise troponin rise had higher pre-exercise heart rates (p=0.03), and higher maximum heart rates (p=0.004).
Univariable associations with a postexercise troponin rise: clinical, biomarker and MRI characteristics
Biomarker
The percentage of patients with HCM with a pre-exercise troponin level ≥14 ng/L tended to be higher than observed in patients without a rise (p=0.07).
Imaging
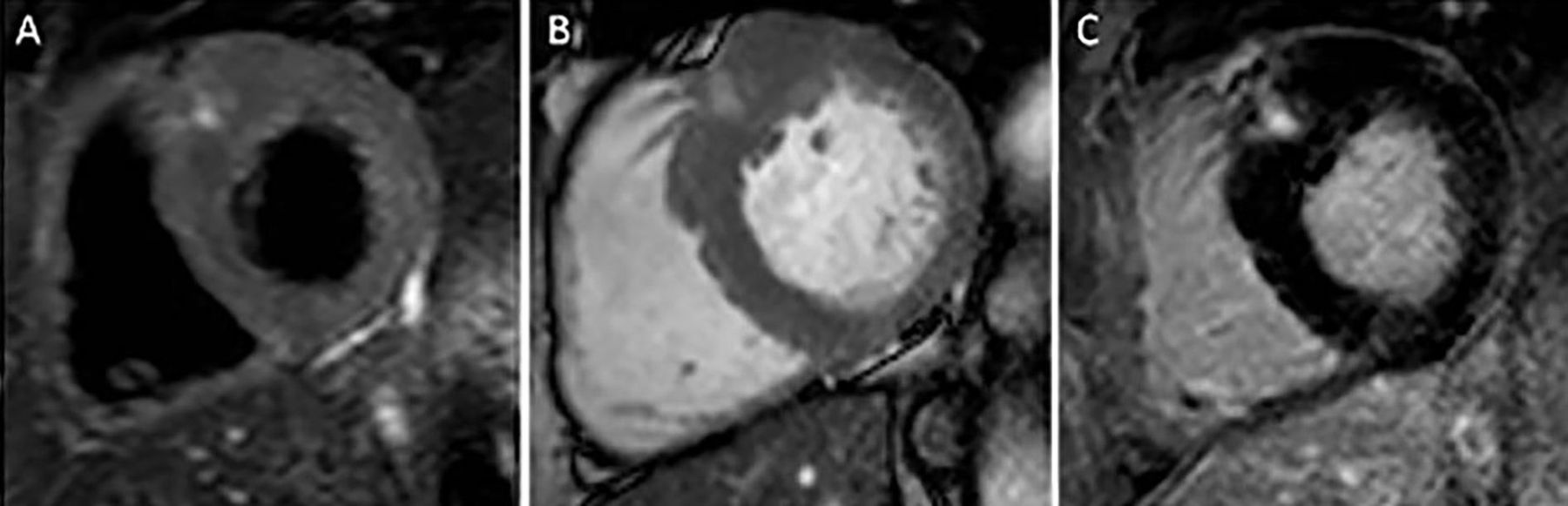
In 109 of the 127 patients with HCM, CMRi was performed. Median MWT was 20 mm (15-23 mm) in patients with a rise, and 17 mm (14–20 mm) in patients without (p=0.023). LGE was present in 85% (17/20) of patients with and in 57% (51/89) without a rise (p=0.02). HighT2 was seen in 65% (13/20) and 19% (15/79) (p<0.001), respectively. A typical example of a patient with signs of HighT2 is shown in figure 1. Of the 28 patients with evidence of HighT2, a postexercise troponin rise was seen in 46% (13/28), which was more than four times more often than in patients without HighT2 (9.9%; 7/71). In figure 2, pre-exercise and postexercise troponin levels are displayed according to the number of myocardial segments with HighT2. There were more patients with a postexercise troponin rise in the groups with 1 or 2, and 3 or more HighT2 myocardial segments as compared with patients with HCM without signs of HighT2 (p<0.001).

Example of a patient with elevated signal intensity on T2-weighted imaging. Panel A: T2-weighted image; panel B: cine image; panel C: T1-weighted image showing late gadolinium enhancement in the hypertrophied part of the basal septum.

{kind=link}
{kind=link}
Highly sensitive cardiac troponin T values according to number of segments with HighT2 0 segments: 9.9% of patients with HCM with a postexercise rise; 1–2 segments: 50%; 3 or more segments: 43%; p value for difference between groups<0.001. HighT2, elevated signal intensity on T2-weighted imaging.
In multivariable logistic regression analysis, only the presence of HighT2 was independently associated with a postexercise troponin rise (OR 7.9; 95% CI 2.7 to 23.3; p<0.001) (table 4).
Postexercise troponin rise in HCM: multivariable logistic regression
Discussion
This study is a report on postexercise troponin release in the largest HCM population to date and is the first to describe its determinants. A postexercise troponin rise occurred in about 20% of patients with HCM, which was almost five times more frequent than in mutation carriers. According to our expectation, we observed a clear association with heart rate and maximal wall thickness, which fits into the classical concept that increased oxygen demand may elicit postexercise injury in the setting of hypertrophy. However, our CMR findings provide important new insights in the underlying pathophysiology. Independent of other factors, such as LV mass, HighT2 identified a specific group of patients with HCM especially vulnerable for further injury. Appreciating that HighT2 has been suggested to reflect an active disease state of HCM, the present study gives rise to the hypothesis that (repetitive) episodes of high oxygen demand may result in ‘bouts’ of troponin release. In the context that the impact of exercise in HCM is currently unknown, our findings may stimulate future research towards more individualised recommendations regarding exercise.
Troponin release in HCM
With regard to troponin status under resting conditions, various mechanisms have been implicated to explain detectable concentrations in different sets of populations. Whereas in HCM some of these mechanisms may be disease-specific, there will also be an overlap with other patient populations, and even with healthy individuals.20–22 In the community dwelling population, there is a clear association between LV mass and the observed baseline hs-cTnT concentration.22 Also, in HCM, there is an association between measures of LV hypertrophy and baseline cTnT.4 In HCM, however, cardiac hypertrophy is accompanied by impaired myocardial structure and function, with myocyte disarray and inefficient energy utilisation. In addition, perfusion abnormalities and impaired microvascular function are also part of the clinical picture.23 These characteristics are additional conditions that may contribute to troponin release, which may become especially apparent in situations of high oxygen demand, such as exercise. Appreciating that postexercise troponin rises are also observed in healthy individuals,16 a group of mutation carriers without hypertrophy served as a reference. Exercise intensity was markedly higher in this control group and can be considered a well-known determinant of postexercise troponin.16 Despite the difference in exercise intensity, we observed a fivefold higher rate of postexercise troponin rises in the patients with HCM, which suggests that the underlying pathophysiology specific to the HCM phenotype is the main contributor to exercise-induced troponin release.18
Imaging studies in HCM
In addition to the above-mentioned aspects, several imaging studies have provided more detailed evidence on the processes observed during stress/exercise in HCM. First, stress imaging studies demonstrated that although hypoperfusion is most often seen in areas of hypertrophy, it also occurs in other myocardial areas, both at rest and during stress, which implicates another mechanism than increased oxygen demand due to hypertrophy.10–12 Second, a previous study on exercise in HCM addressed the issue of inefficient energy utilisation and demonstrated that exercise worsened the energy deficit in these patients, independent of hypertrophy and fibrosis.24 This aspect may have contributed to our observation that a troponin rise after exercise is not confined to patients with the highest LV mass and/or wall thickness.
Interestingly, in multivariable analysis, HighT2 was found to be the only variable associated with a postexercise troponin rise. Considering that 80% of patients did not show biomarker signs of postexercise injury, higher oxygen demand by itself is not the key driver of myocardial injury after exercise. The underlying state of cardiac disease seems an important predisposing factor to develop a postexercise troponin rise.
Under resting conditions, there is a strong association between hs-cTnT and HighT2. HighT2 is considered to represent an active state of disease, with recently sustained myocardial injury.4 13 With CMRi performed prior to the bicycle test, our findings support the concept that patients with HCM with signs of oedema represent a group with active disease, vulnerable to new injury. As HCM is highly heterogeneous, the occurrence of postexercise troponin rises in patients with HCM with HighT2 is subject to variation among individuals. In view of this, HighT2 remains present for a longer period of time, and repeated exercise with different intensities will cause troponin releases on some, but not all occasions.
These findings may contribute to further improve the characterisation of different disease states with the use of CMRi, as previously suggested by others.11
Implications
This study provides insights that may contribute to further investigate the role of exercise in HCM. At present, available information is limited and guideline recommendations lack high-level scientific support.25 Several observations have recently made experts to suggest that the risks of exercise are low.26–28 However, the associated risks and benefits in this patient population are uncertain, and guidance to differentiate for whom exercise may be beneficial, or potentially harmful, is lacking.25
Importantly, whereas about 80% of patients did not show a postexercise rise in troponin, HighT2 could identify a subset of patients who were vulnerable to additional injury in almost 50%. The clinical potential of this differentiation requires further follow-up, which is supported by observations that HighT2 has been linked to a higher risk of non-sustained ventricular tachycardia and syncope.29 30 Ultimately, this distinction has the potential to contribute to more individualised recommendations.
First, however, additional information is needed with regard to the clinical meaning of a postexercise troponin rise, in terms of progression of disease and prognosis. In this regard the associations that we found are first-time findings that need to be substantiated in larger-sized cohorts with follow-up CMRi to assess a potential causal relationship between postexercise troponin rises and imaging signs of progressive myocardial disease. Therefore, further research is warranted to assess the association with outcomes such as, for example, extension of LGE, LV deterioration and clinical endpoints like heart failure and (arrhythmic) death.
In case of a demonstrated association with adverse outcome, this could pave the way for future research. As far as potential interventions are concerned, we previously reported in a pilot study that postexercise release of troponin in HCM could be blunted with the use of a beta-blocker.17 Future developments may include defining individualised exercise thresholds based on intensities that result in postexercise injury. Appreciating the current gaps in knowledge for an every-day issue like exercise, future initiatives to more personalised, informed decision making are eagerly awaited.
Limitations
Although this is the largest prospective, controlled study addressing the impact of exercise on troponin release in HCM, the sample size is still modest and associations of other variables with a postexercise troponin rise may have gone undetected. As an example, differentiation according to mutation type could prove of interest as some mutations might do worse than others. Second, we excluded patients with a history of cardiovascular disease and/or septal reduction therapy; thus, findings cannot be generalised to the entire HCM population.
In retrospect, a more extensive CMRi protocol including adenosine, T1 and T2 mapping would have provided more elaborate tissue characterisation, which might have resulted in additional insights. However, at the time of study design, the latter two techniques were not available.
With our current knowledge on release patterns of hs-cTnT after exercise, the timing of blood samples 6 hours postexercise may have been rather late. However, at the time of study design, data on troponin, exercise and HCM was limited.
Conclusion
In patients with HCM, a postexercise troponin rise is observed in about 20%, almost five times more frequent than in mutation carriers without hypertrophy. In the latter, exercise was well tolerated with only a few cases showing a limited rise in the level of troponin. In patients with clinical HCM, maximal wall thickness and heart rate were associated with the occurrence of a rise, but the only independent association was found for the presence of HighT2 at CMRi prior to exercise. These findings give rise to the hypothesis that in HCM, episodes of high oxygen demand may elicit additional myocardial injury particularly in case of an active state of disease.
Key messages
What is already known on this subject?
In hypertrophic cardiomyopathy (HCM), troponin and high signal intensity on T2-weighted (HighT2) cardiovascular magnetic resonance imaging (CMRi) are both markers of myocardial injury. A resting troponin elevation is seen in about 25%–50% of patients, especially in case of HighT2 (oedema). The interplay between exercise in HCM and development of disease remains uncertain. An increase in troponin after exercise has been reported, but how often this occurs, and its potential determinants are unknown.
What might this study add?
A postexercise troponin rise was observed in about one out of five patients with HCM, five times more frequent than in mutation carriers without the phenotype. In line with the classical concept of hypertrophy and increased oxygen demand, heart rate and maximal wall thickness were univariable determinants. The only independent association was found for HighT2. This shows that exercise per se does not cause injury in the majority of patients with HCM, and that CMRi may identify a particularly vulnerable subgroup.
How might this impact on clinical practice?
These data provide the first indication that the injury-response to exercise differs among patients with HCM and that patients with a more active state of disease (HighT2 on CMRi) are more vulnerable. These findings may stimulate future research that could contribute to more individualised recommendations with regard to exercise (intensity) in HCM.
References
Footnotes
Contributors All authors have significantly contributed to the design and conception of the study, and they participated in the collection of data and analysis of the data. All authors have reviewed and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All provided data included in the article cannot be traced back to individuals that participated in the study.