
Discussion of diagnosis
AIN is a well-known complication of therapy with a number of medications, including proton pump inhibitors,[1] NSAIDs, and antibiotics such as vancomycin,[2,3,4] cephalosporins, sulphonamides,[5] and several penicillin derivatives.[6,7,8,9,10] Meticillin (formerly methicillin) is the penicillin derivative most commonly reported as associated with nephritis, with up to one-third of exposed patients developing the complication.[10] By contrast, nafcillin, a semisynthetic penicillin extensively used as the drug of choice for treatment of a number of meticillin-sensitive S. aureus (MSSA) infections such as endocarditis, catheter-related infections, and complicated soft tissue infections,[11,12] was reported to be an unlikely cause of AIN in 1980.[13] A prospective analysis of 210 consecutive patients given nafcillin at the University of California, San Francisco, indicated the complete absence of clinically significant nephrotoxicity.[13] Furthermore, few suspected cases of nafcillin-associated interstitial nephritis have been reported over the past 25 years.[6,9] The recent clinical experience at the institution where the present case was treated, however, suggests that this 'rare' complication of nafcillin might be underappreciated.
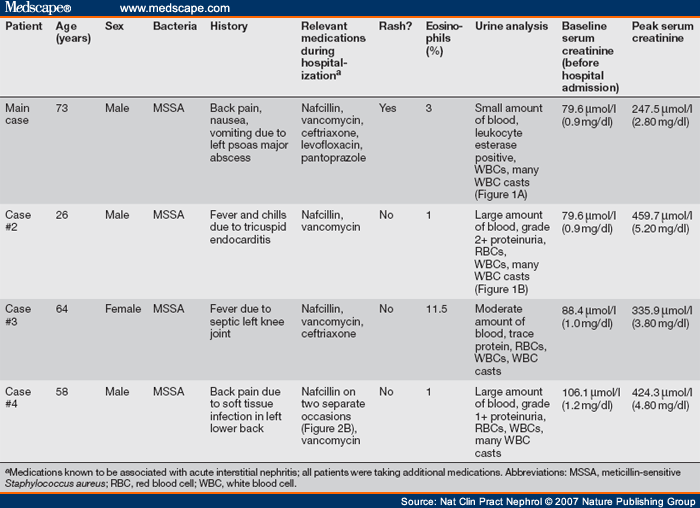
Over the course of 1 year, a total of four patients with MSSA infections presented to the same institution and developed acute kidney injury (AKI) most likely secondary to nafcillin-associated AIN (see Table 1 ). Discontinuation of nafcillin (while other medications were continued) resulted in improvement in kidney function in all cases. In one case (case #4 in Table 1 ), re-exposure to nafcillin led to a relapse of renal inflammation (Figure 2B). The cases reported here provide compelling data to support the diagnosis of nafcillin-associated AIN as the primary cause of each patient's AKI and they highlight the important diagnostic clues that can be used to establish this diagnosis.
Sterile pyuria with white blood cell casts and kidney dysfunction were universal findings in all cases. With these abnormalities, the diagnosis of drug-induced AIN seemed probable. While it is well known that multiple classes of drugs can precipitate AIN,[1,2,3,4,5,6,7,8,9,10] careful review of the medication administration records demonstrated a clear relationship between nafcillin initiation and the development of AKI in each case. This temporal association was not as apparent for other medications known to cause AIN, such as vancomycin, ceftriaxone and pantoprazole. In each case, kidney function improved with cessation of nafcillin (Figure 2). A strong preference of the infectious disease consultant for use of nafcillin to treat the S. aureus infection in case #4 led to this antibiotic being restarted in this patient. Re-exposure to nafcillin promptly led to a relapse of kidney inflammation (Figure 2B). Additionally, both hematuria and proteinuria were seen in all four patients. Previous case reports of nafcillin-associated AIN have also described hematuria and proteinuria,[6,9] and these findings are also common in those receiving meticillin.[8] Finally, rash (which occurred in the main case) and peripheral eosinophilia (which occurred in case #3) have both been reported with nafcillin[6,9] and meticillin.[8] While a kidney biopsy remains the gold standard for a pathological diagnosis of AIN, the diagnosis can also be based on strong clinical evidence. In each case presented here, pyuria with frequent white blood cell casts was the dominant urinary finding as the GFR declined. No red blood cell casts or 'muddy brown' casts were present in any of the cases. These observations, combined with the timing of nafcillin exposure, made the clinical diagnosis of nafcillin-induced AIN the most compelling. Kidney function promptly improved in each patient with cessation of nafcillin exposure, obviating the need for renal biopsy. Gallium scans were not pursued in the diagnostic work-ups as their utility in the diagnosis of drug-associated AIN has not been clearly established.[14]
Nat Clin Pract Nephrol. 2007;3(8):456-461. © 2007 Nature Publishing Group
The authors declared no competing interests.
Cite this: Four Cases of Nafcillin-Associated Acute Interstitial Nephritis in One Institution - Medscape - Aug 01, 2007.


Comments