
A new analysis of health inequities in the United States shows that every state has deep racial and ethnic disparities in the performance of their health care systems.
The report released Thursday by the Commonwealth Fund analyzed 25 indicators that track health outcomes, health care access, and quality of care provided for five racial and ethnic groups. It found dramatic disparities for Black, Hispanic, and Indigenous Americans, even in Rhode Island, Massachusetts, Connecticut, Hawaii, New Hampshire, and New York — the states considered to have the best overall health care performance. In all states, White and Asian residents had the best health outcomes.
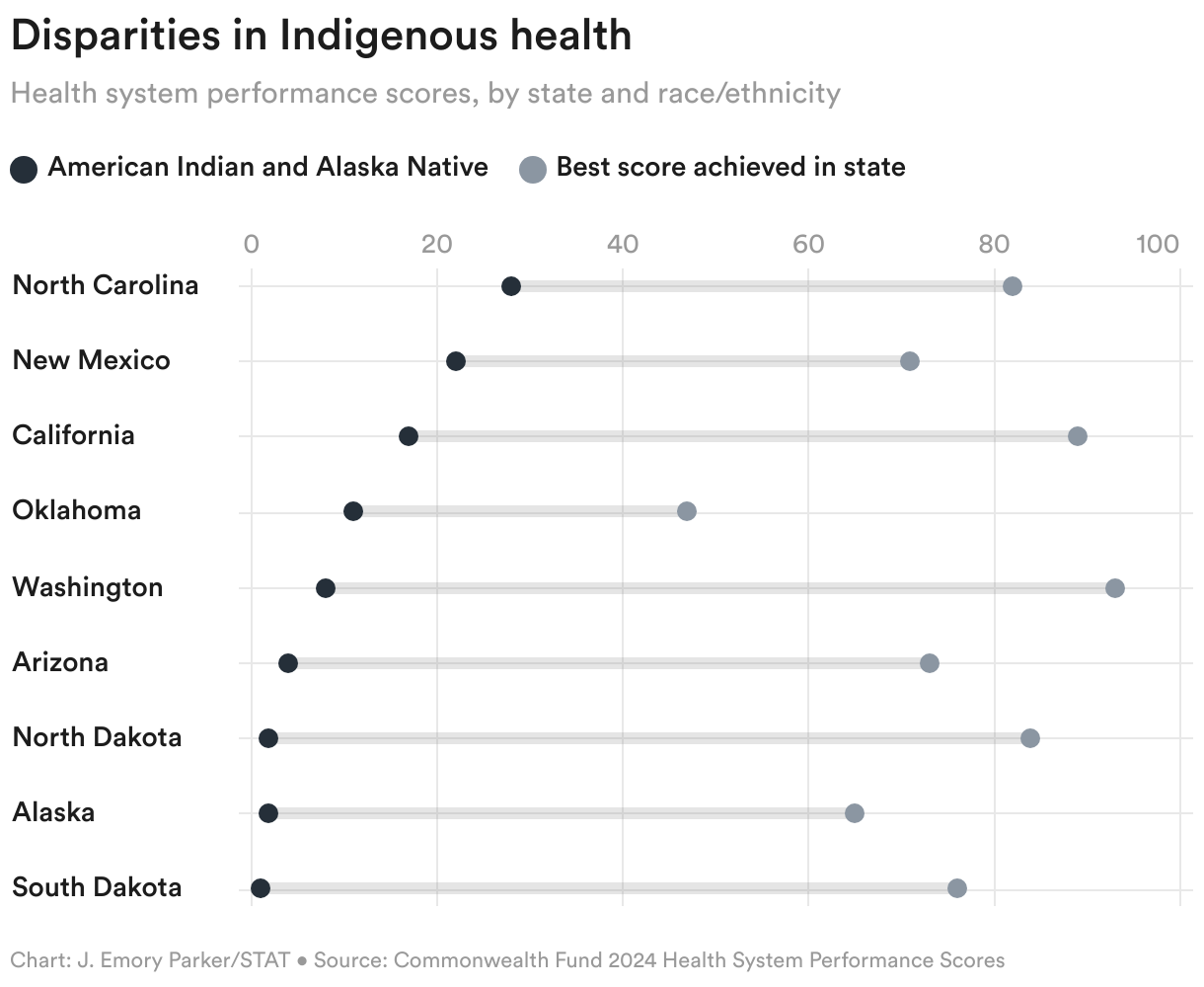
“Health equity does not exist in any state in the U.S.,” said David Radley, a co-author of the report and senior scientist at the Commonwealth Fund. Analyses of health system performance that average all groups together, he said, mask the gaps that exist within each state. The report also made clear that the health disparities experienced by different racial and ethnic groups were not universal but differed by state: Some, like North Carolina, had better outcomes than other states for Indigenous people, but worse outcomes than other states for Hispanic people.
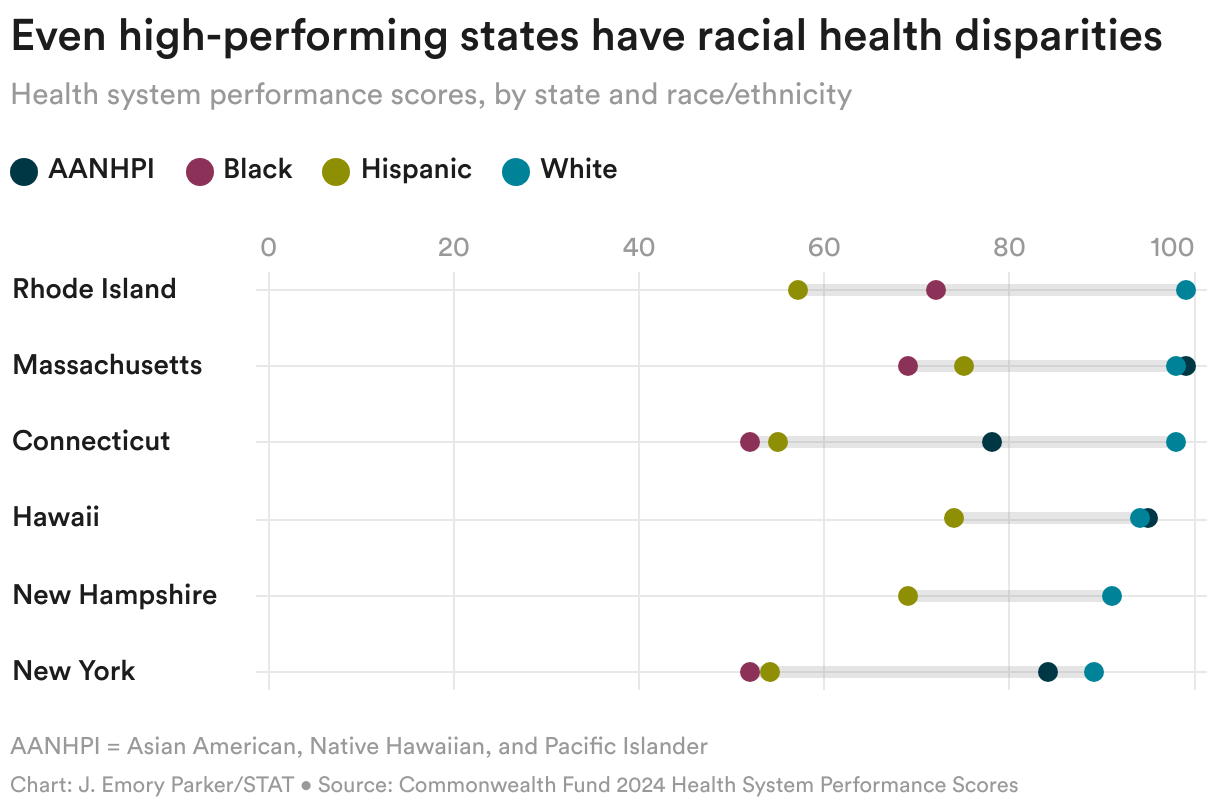
States with generally good health outcomes on average, but far poorer health outcomes for Black residents, included Minnesota, Illinois, and Wisconsin. Only six states (Rhode Island, Massachusetts, Maryland, Connecticut, Delaware, and New York) had health outcomes of Black residents that were above the average performance for all states, but these outcomes were still far lower than the top performing groups in each of those states.
The states with the worst outcomes for Hispanic people relative to higher performing groups were Maryland, North Carolina, and South Carolina. Hispanic people in nearly all states had low rates for premature mortality that matched those of white people, with the exception of several southwestern and mountain states where premature deaths were far higher: New Mexico, Arizona, Colorado, Texas, and Wyoming. Report authors said more analysis was needed to understand why those states differed, but said insurance access and challenges of providing health care in rural settings likely played a role.
The data came from 2021 and 2022 and therefore included deaths from Covid-19, which struck Black, Hispanic, and Indigenous populations at higher rates. The premature death rate was higher for Black populations in nearly every state; in six southern and south-central states (Arkansas, Mississippi, Louisiana, Tennessee, Kentucky, and Missouri), premature death rates for both Black and white residents were higher than in other states.
The report revealed a stark rate of premature death for Indigenous people, who in several states — South Dakota, Wyoming, Montana, and North Dakota — had the highest premature death rates of any groups in any state, with deaths caused largely by conditions that were treatable.
The “findings shine light through the many holes in the U.S. health care system, especially for those who have brown or Black skin,” said Siobhan Wescott, an Alaska Native physician and professor of American Indian health at the University of Nebraska Medical Center, who was not involved in the new report. “It’s time to reconsider our priorities or reports like this will be commonplace.”
Leaders of the Commonwealth Fund said they hoped the analysis would encourage states and health systems to consider policies and investments that make health care more equitable. Measures that could reduce disparities, they said, include supporting primary care physicians, social service providers, and community health workers in Black, Hispanic, and Indigenous communities and providing more and better health insurance.
“Insurance coverage is a key part of this,” said Laurie Zephyrin, a physician and senior vice president of the Commonwealth Fund. “25 million people in the U.S. are still uninsured and they are primarily people of color.”
Medicaid expansion under the Affordable Care Act is one way to increase the number of people insured in a state. Several states, including Missouri, Nebraska, Oklahoma, Utah, South Dakota, and North Carolina have ushered in Medicaid expansion in recent years, noted Sara Collins, a senior scholar and vice president at the Commonwealth Fund, adding that she expected to see health outcomes begin to improve in those states as a result.
Joseph Betancourt, the Commonwealth Fund’s president, said he hoped the report would inspire states to look more deeply at their own disparate health outcomes, to understand regional differences that may be at play, and to learn from states that had fewer disparities. “If you don’t look under the hood,” he said, “you won’t identify where you’re failing people and where you’re leaving people behind.”
This is part of a series of articles exploring racism in health and medicine that is funded by a grant from the Commonwealth Fund. Our financial supporters are not involved in any decisions about our journalism.
About the Author Reprints
To submit a correction request, please visit our Contact Us page.










STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect